Case report
MT, 7-month-old female, was referred to our practice in March by the Royal Children’s Hospital for contact lens fitting. She was due to have her intraocular lenses and vitreous removed from her eyes the following month. She has a family history of lens subluxation (i.e. the lens inside the eye becoming loose and dislocating), including her affected father who is also aphakic (without an intraocular lens). The ophthalmologist discovered MT’s crystalline lenses to be temporally subluxed in both eyes causing secondary congenital glaucoma and buphthalmos (enlarged eye). MT was placed on maximum glaucoma medical therapy including Xalatan nightly, Cosdor twice a day, Atropt daily and Diamox three times a day to help reduce her intraocular pressure (IOP) prior to the surgery.
After a lengthy discussion detailing the available corrective options available for paediatric aphakia, it was decided to proceed with rigid contact lenses.
MT was fitted with the flattest (BOZR = 8.20mm) and largest (TD = 13.0mm) rigid contact lens available in our aphakic diagnostic kit. Sodium fluorescein analysis revealed a steep fit with central pooling and a large air bubble. The lens diameter appeared to be of sufficient size. Most of our contact lens fittings can be performed in office, however MT is outside the standard range of eye sizes and shapes due to her buphthalmos. At Eyetech we have high tech instrumentation including the Pentacam-AXL Wave and the Medmont Meridia that can measure the shape of the ocular surface, however these are not possible to perform on a young child as they are required to sit still for a couple of seconds, which is a long time for a baby! Fortunately, as we had seen MT prior to surgery, we could ask the surgeons to measure her corneal curvature. Post-surgery, her specialist provided retinoscopy results of +12.50D and K readings of +40.0D (8.44mm). Initial contact lens parameters of 8.65/13.50/+18.00D were then ordered as a starting set with intent to modify.
MT’s surgery was uneventful but her post-surgical IOP remained elevated at 30mmHg. Ocular hypertension (OH) is a common post-surgical complication in children, a study by Lin (2013) indicated that 17% of aphakic eyes are diagnosed with ocular hypertension in the first year following surgery, and 80% of those are diagnosed within the first month. The duration of OH was an average of 30 days, but 24% recur over the first year if diagnosed within the first month. Close monitoring of the IOP in the post-operative period is essential.
At the delivery of the lenses, assessment of the lens fit and prescription was quite challenging due to excessive lacrimation and photosensitivity due to corneal clouding. Accurate retinoscopy was not possible with either the optometrist or ophthalmologist. It was decided to perform an examination under general anaesthesia (EUA) for accurate IOP and optic nerve assessment. Jamie and Victor attended to assess the contact lens fit during anaesthesia.
The EUA was conducted in June. Fortunately, the IOP had reduced to R 14mmHg and L 15mmHg and the optic nerves and angles appeared healthy (Figures 1a, 1b, 2a, 2b). Axial lengths were R 25.60 and L 25.81mm and central corneal thickness were R 596 and L 571 microns. The lenses were placed on the eyes and assessed with sodium fluorescein. There were large bubbles under each lens L>R, indicating a steep fit (Figures 3a and 3b). Keratometry readings revealed corneal curvatures of 36.0D (9.38mm) in each eye and retinoscopy +15.0D. A flatter set of lenses were ordered with the parameters R 9.1/14.00/+21.50 and L 9.30/4.00/+21.50

Figure 1a - R Fundus photo

Figure 1b - L fundus photo
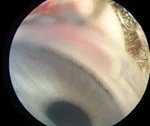
Figure 2a - R Angle photo
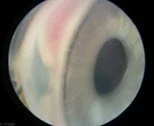
Figure 2b -L Angle photo
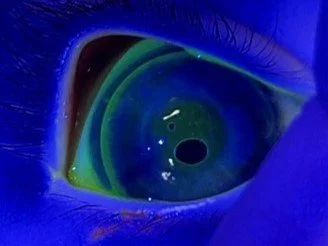
Figure 3a - R RGP in situ with NaFl
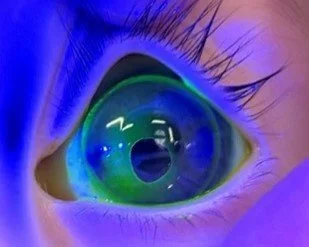
Figure 3b - L RGP in situ with NaFl
At the one-month follow-up, MT was comfortable and visually engaged with the new lenses. The lenses appeared well fitting with good alignment fit with good edge clearance. The lenses appeared stable on the eyes and well centred, the retinoscopy reflex was clear and neutralised at 40cm – i.e. over-corrected by 2.5D. Her eye pressures remain stable at R 14mmHg and L 19mmHg .
MT was also fitted with spectacles which were kindly donated through the OneSight Essilor Luxottica Foundation. The foundation is a global charity working to reduce uncorrected poor vision by improving access and education to those in need. More information is in the link below.
MT has undergone genetic testing to confirm FBN1-variant, which is strongly associated with Marfan’s syndrome. Given this diagnosis, her axial length measurements and congenital glaucoma, MT will require routine serial monitoring for progression of myopia and glaucoma.
This was a challenging case due to buphthalmos induced from the glaucoma, resulting in a corneal diameter significantly larger and corneal curvature flatter than norms, meaning all our fitting lenses were far too flat. At Eyetech we typically perform contact lens fitting in office, however with cases like this our typical ‘educated’ SWAG (sweet wild-ass guess) technique falls apart. Being able to attend an EUA was highly valuable in this situation to ascertain ocular parameters we would not be able to attain in an alert baby, and allowed for better visualisation of the lens fit and power for MT.
References
Lin, H., Chen, W., Luo, L., Zhang, X., Chen, J., Lin, Z., Qu, B., Zhan, J., Zheng, D., Zhong, X., Tian, Z., Liu, Y., & Study Group of CCPMOH (2013). Ocular hypertension after pediatric cataract surgery: baseline characteristics and first-year report. PloS one, 8(7), e69867. https://doi.org/10.1371/journal.pone.0069867